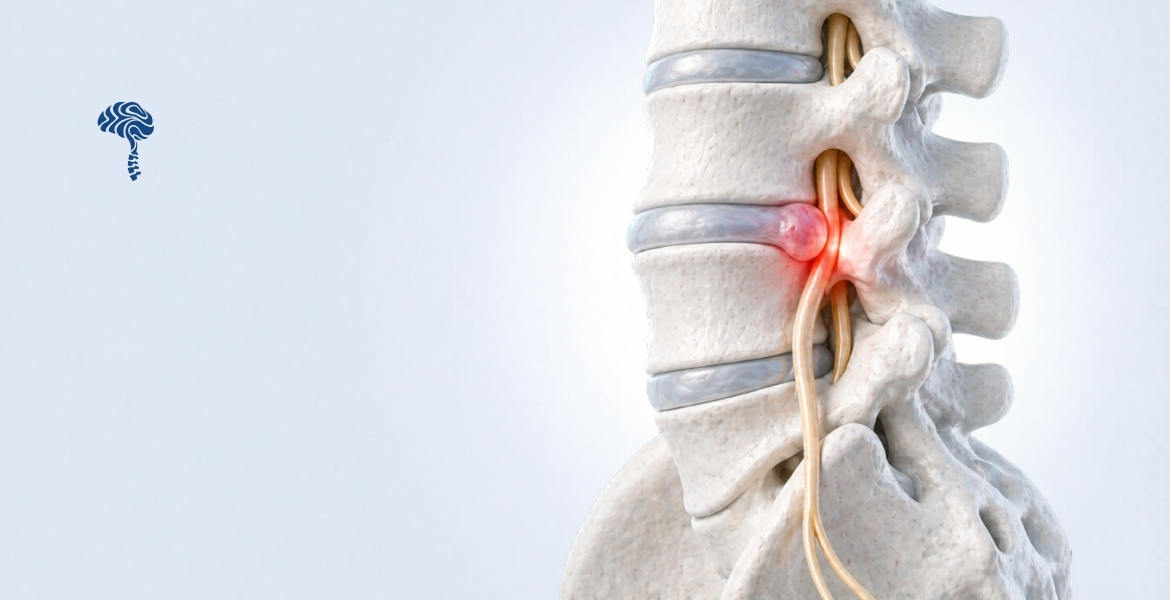
What Is Lumbar Disc Herniation?
Lumbar disc herniation occurs when the nucleus pulposus — the gel-like centre of an intervertebral disc — pushes through a tear in the outer fibrous ring (annulus fibrosus). This displaced material can press on nearby nerve roots, triggering pain that radiates far beyond the lower back.
It is one of the most common causes of sciatica and affects roughly 1–3% of adults each year, with peak incidence between the ages of 30 and 50.
Common Causes
- Age-related disc degeneration — discs lose hydration and elasticity over time, making them more susceptible to rupture.
- Improper lifting mechanics — flexing the spine under load dramatically increases intradiscal pressure.
- Repetitive microtrauma — jobs involving prolonged sitting, driving, or vibration accelerate disc wear.
- Obesity — excess body weight increases axial load on lumbar segments.
- Genetic predisposition — collagen composition of the annulus is partly inherited.
Recognising the Symptoms
Symptoms vary depending on the level of herniation and which nerve root is compressed:
- Sharp or burning pain radiating from the buttock down the leg (sciatica)
- Numbness or tingling in the thigh, calf, or foot
- Muscle weakness — difficulty standing on tiptoe (S1) or lifting the foot (L4/L5)
- Pain that worsens with sitting, coughing, or sneezing
- In severe cases: bladder or bowel dysfunction — a medical emergency (cauda equina syndrome)
“Pain that radiates below the knee is the most reliable clinical indicator of true nerve root compression, not just disc bulge.” — Dr. Jagadeesh, Consultant Neurosurgeon
Diagnosis
A thorough neurological examination combined with MRI of the lumbar spine remains the gold standard. CT myelography is reserved for patients who cannot undergo MRI. Plain X-rays alone do not visualise disc material.
Treatment Options
Conservative Management (First 6 Weeks)
- Relative rest — avoid provocative positions; maintain gentle activity
- NSAIDs and short-course oral corticosteroids for acute inflammation
- Structured physiotherapy: core stabilisation, McKenzie exercises
- Epidural steroid injections for refractory radicular pain
Surgical Intervention
Surgery is indicated when conservative measures fail after 6–12 weeks, or immediately in cases of progressive neurological deficit or cauda equina syndrome.
- Microdiscectomy — gold standard; removes the herniated fragment through a small incision with microscopic magnification
- Endoscopic discectomy — minimally invasive, reduced soft-tissue disruption, faster recovery
Over 90% of properly selected patients experience significant relief following microdiscectomy.